![]() Optimization of Intraoperative CT with Automatically-Registered Surgical Navigation
Optimization of Intraoperative CT with Automatically-Registered Surgical Navigation
Tanya Verma, Wenbo Gong, Nick Norman, James Keck, William van Kampen
Keywords: intraoperative CT, IGS, navigation, registration, computed tomography, image guided surgery, Xoran, xCAT, Fiagon
Abstract: Intraoperative CT (iCT) provides valuable updated imaging during surgery to support image- guided surgery (IGS) of the paranasal sinuses and skull base. Automated registration, with potential to improve IGS accuracy and optimize workflow, has been missing to make iCT practical during surgery. This study utilized a new scan-to-navigation automated protocol. The study aimed to optimize image quality, speed, ease of use, and patient radiation dose. A series of phantom and cadaveric tests were conducted using a Xoran intraoperative CT scanner coupled to a Fiagon surgical navigation system. The results show that using a low dose imaging technique, and an automated registration method, it is possible to provide high quality images, with submillimeter IGS “accuracy” at the skull base in about two minutes and at an objectively low effective dose, and equivalent to a chest x-ray.
Methods: Intraoperative CT scans were obtained from a Xoran xCATTM (Xoran Technologies, Ann Arbor, MI), and transferred to a Fiagon IGS system (Fiagon GmbH, Berlin). CT parameters were varied including x-ray tube current, number of projection frames, reconstruction voxel size and output slice thickness. Tube voltage of 120kVp was held constant. A head phantom containing radio-opaque test points was used for field tracking accuracy measurements. A registration tool containing radiopaque fiducials and a tracking sensor was placed on the phantoms bridge of nose during imaging to facilitate the automatic registration. For each test, the reconstructed volume of the head phantom was transferred via DICOM to the Fiagon IGS. The fiducial registration error (FRE) was calculated as a root mean square (RMS) sum of deviations from expected fiducial positions. To evaluate target registration error (TRE), test points at the forehead (near the registration cage) and skull base of a head phantom were touched with a tracked probe. TRE was found by measuring the distance from each radio-opaque fiducial point to the tip of the navigated Fiagon FlexPointerTM, as displayed on the IGS screen. Error measurements were recorded in axial and sagittal planes. For two of the nine tests error measurements were recorded by two individuals to give an estimate of interrater variability. All other tests were measured by a single individual. The total time to acquire a CT scan, reconstruct, transfer, register, and resume active navigation was recorded to assess the speed of the entire workflow. A cadaveric specimen was imaged with identical techniques to enable assessment of image quality.
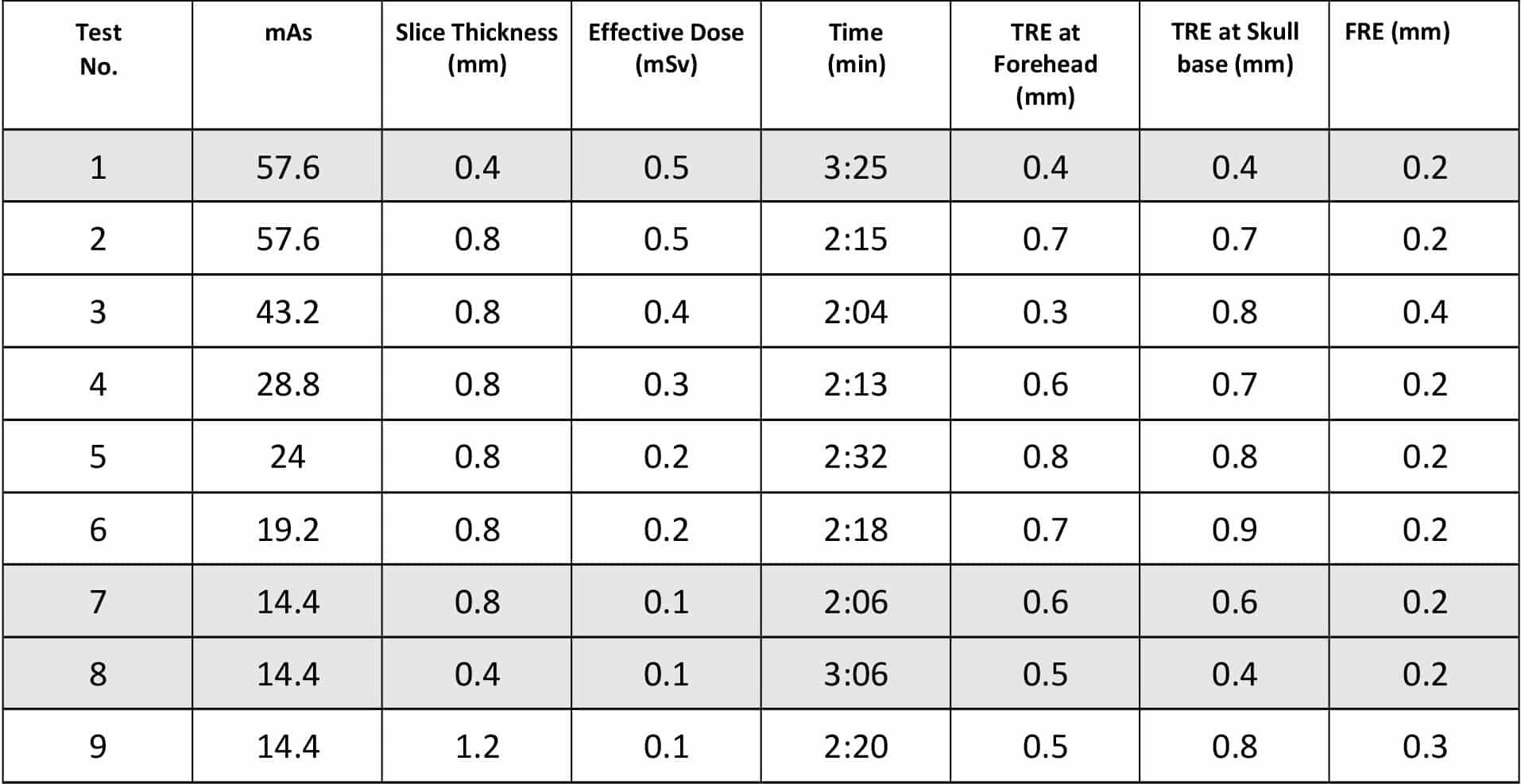
Results: The table below contains test parameters and results. The standard protocol is Test 1. Other protocols offer considerable dose and speed improvement. Test 7 enables the fastest workflow, while Test 8 offers the highest accuracy; both of these are at a quarter of the standard dose. The maximum TRE measurements in the entire series of tests was a deviation of 1.1 mm at the skull base. None of the other TRE measurements exceeded 1.0 mm. The maximum of the inter-rater differences in error measurements in test 8 and 9 was 0.3 mm and the mean of the inter-rater differences was 0.16 mm.

Figure 1: Experimental set-up showing the Xoran xCATTM intraoperative CT scanner (right), Fiagon navigation system field generator (left), automatic registration device, located on phantom forehead.
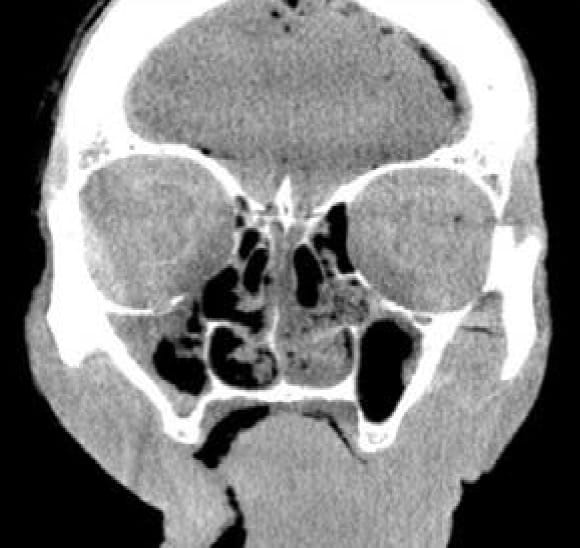
The following are images and figures of a human cadaver head acquired with the xCATTM using the protocols in tests 1, 7 and 8 showing the coronal and sagittal views. The image noise measurements were made by calculating standard deviation (STD) in a region of interest (ROI) drawn in the soft tissue, near the left temporal bone in an axial slice.
|
Standard Protocol (TEST 1) Technique: 120 kVp, 6 mA Slice Thickness: 0.4 mm Effective Dose: 0.5 mSV Noise (STD): 30 HU |
 |
 |
| Low Dose, Fast (TEST 7) Technique: 120 kVp, 3 mA Slice Thickness: 0.8 mm Effective Dose: 0.1 mSV Noise (STD): 40 HU |  |
 |
|
Low Dose, Standard Resolution (TEST 8) Technique: 120 kVp, 3 mA Slice Thickness: 0.4 mm Effective Dose: 0.1 mSV Noise (STD): 50 HU |
 |
 |
Conclusion: As expected, the results show that workflow time is inversely related to slice thickness of the image data volume. Increasing slice thickness also increases the measured TRE; however, further study is needed to determine if the difference is clinically relevant. While image noise increases with lowering effective dose, the perceived image quality remains suitable for clinical use at 0.1 mSv. Additional clinical evaluation may be warranted to support this finding.
Summary: Jointly optimizing the CT and IGS can lead to meaningful advantages for accuracy, patient safety and speed. Imaging parameters affect the speed and accuracy of the IGS in addition to the image quality and radiation dose. With image-based registration, it is possible to acquire intraoperative CT and resume IGS navigation quickly and automatically. With a modified technique, dose can be reduced while preserving adequate visual image quality and navigation accuracy. The optimal settings will depend on the specific application and clinician preferences. A low-dose protocol provided high quality images, with submillimeter navigation accuracy at the skull base in about two minutes and at an effective dose of 0.1 mSv, approximately equivalent to that of a chest x-ray.
Acknowledgement: We would like to thank Fiagon GmbH for providing us their surgical navigation system and for the support and assistance in integrating it with xCATTM to perform the tests.
| Download the White Paper PDF. |
60135-02-2017